Copyright Goodheart-Willcox Co., Inc.
Chapter 2 Career Skills in Health Informatics
55
Filing
While most medical records are stored electronically these days,
workers may still need to access paper records that are maintained as a
back-up storage system. Patient records must be easy to store and fi nd so
that patient care and treatment can run smoothly on a day-to-day basis.
Proper fi ling of records can also help avoid potential lawsuits by keeping
all necessary information available for review. Medical records are stored
either alphabetically or by number (numerically).
PR
OC EDUR
E
S
SKILLS
S
K
I
L L
S
P
R E
S
S
K
I
L L
S
R
O
U
R
E
S P P
R
O
C E
D
U
E R
O
C E
D
U
R
E
SUN VIEW MEDICAL MEDICAL HISTORY FORM
(please print/type)
Last Name First Name Middle Name
Date of Birth Sex/Gender Country of Birth
( )
Permanent Address City State Zip Code Telephone
( )
Local Address City Zip Code Preferred Local Telephone
HAVE YOU HAD: YES NO YES NO YES NO
Head Injury with
Unconsciousness
Sexually Transmitted
Disease
Counseling/Mental
Health Treatment
Asthma Malaria Recreational Drug Use
Recurrent Headaches Chicken Pox Tobacco Use
Seizure Disorder Scarlet Fever Alcohol Use
Hearing Loss Hay Fever
# times per week
Recurrent Ear Infections Rheumatic Fever
amount per session
Visual Problems
(other than glasses)
High Cholesterol Exercise:
# times per week
Thyroid Problem Hepatitis A, B, or C Operations / Dates:
Heart Problem/Murmur Diabetes
Kidney/Urinary Tract Problem High Blood Pressure Chronic Health Problems:
Gynecology Problem(s) Digestive Tract Problem
Recent Weight Change Cancer/Tumor/Cyst
Bleeding/Blood Disorder Spinal Cord Disruption Alternative Medicine Practices:
Tuberculosis Eating Disorder
ALLERGIES to Drugs/Medications:
(write NONE if none)
OTHER ALLERGIES
(i.e., environmental):
(write NONE if none)
Routine Medications Taken:
(write NONE if none)
Family Health History
(List father, mother, siblings, spouse/partner and children)
Family Member Age If no longer living, cause of dealth and age of death
HAS ANY FAMILY MEMBER EVER HAD:
(parent, sibling, or grandparent) YES NO Relationship YES NO Relationship
Tubercolosis Asthma
Drug/Alchohol Use Thyroid Disease
Diabetes Seizure Disorder
Kidney Disease Blood Disorder
Heart Disease Cancer
High Blood Pressure Stroke
Arthritis Obesity
OTHER CONCERNS/INFORMATION:
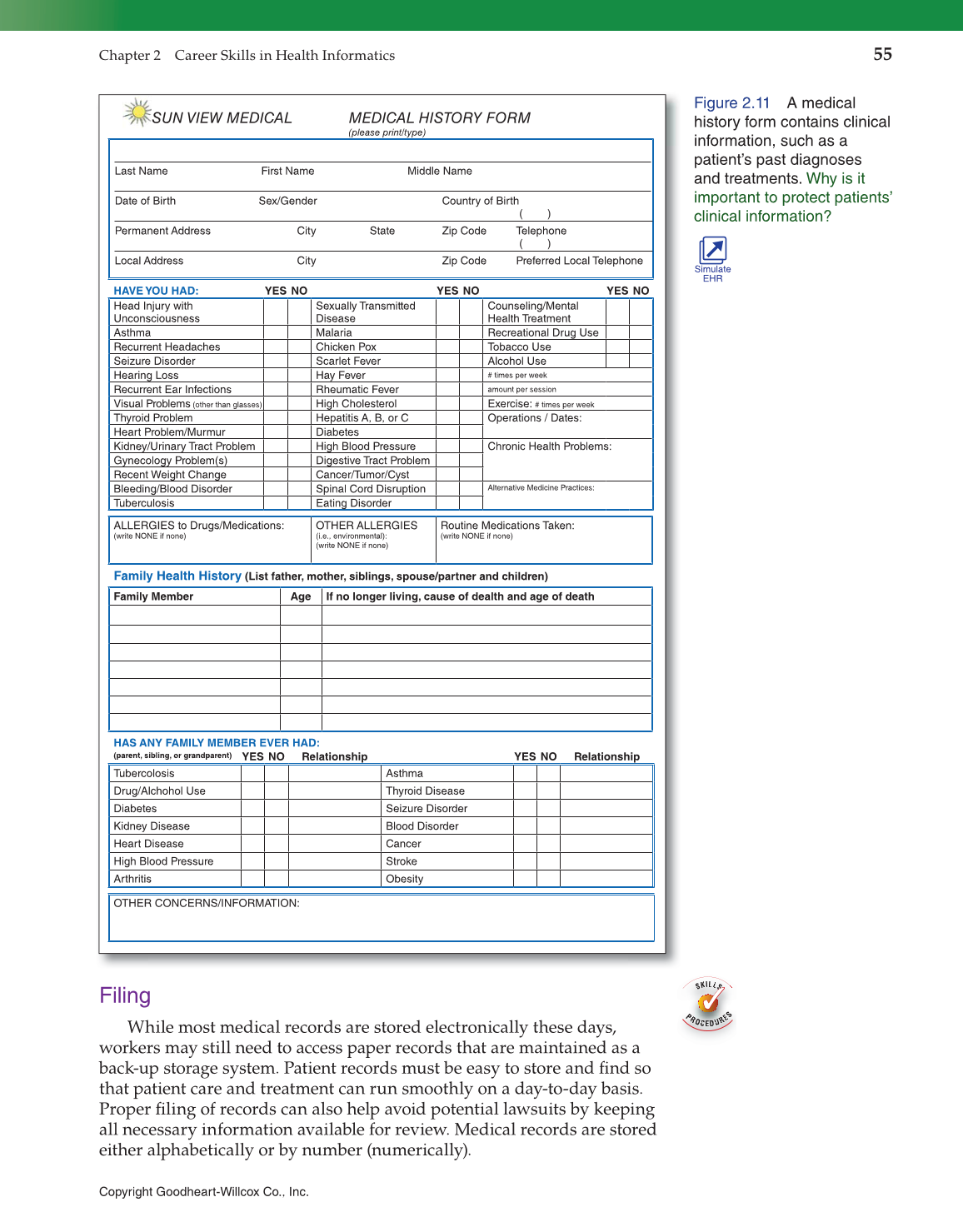
Figure 2.11 A medical
history form contains clinical
information, such as a
patient’s past diagnoses
and treatments. Why is it
important to protect patients’
clinical information?
Simulate
EHR